Bariatric Surgery Cost in India
Written By: Dr. Shivya
Medically Reviewed By: Dr. Ruchika
Last updated: April 08, 2026
Written By: Dr. Shivya
Medically Reviewed By: Dr. Ruchika
Last updated: April 08, 2026
Bariatric surgery cost in India is a fraction of what it costs to get the surgery done in the US, UK, or any other Western country. For example, Sleeve Gastrectomy cost in India starts from $5000 with IndiCure, whereas the cost of the same surgery is around $25,000 in the US, £18,000 in the UK, and $25,000 in Australia.
Bariatric surgery cost in India varies with the type of bariatric surgery procedure chosen, your medical history and condition, surgeon, hospital, and the city where you choose to get the surgery done.
Here's a Quick look at Bariatric surgery cost in India compared to Western countries:
| Procedure | USA ($) | Australia ($) | UK (£) | India ($) |
|---|---|---|---|---|
| Gastric Banding | 25,000 | 30,000 | 12,000 | 6,000 |
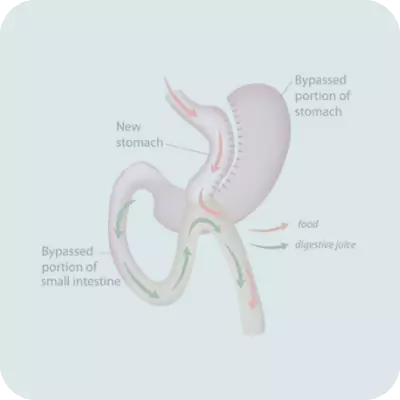
| Gastric Bypass | 30,000 | 35,000 | 20,000 | 6,000 |
| Gastric Sleeve | 25,000 | 25,000 | 18,000 | 5,000 |
| Mini Gastric Bypass | 30,000 | 30,000 | 20,000 | 5,000 |
| Gastric Ballooning | 15,000 | 20,000 | 8,000 | 4,000 |
An important expense when it comes to your bariatric surgery cost in India is your bariatric surgeon's fees. IndiCure recommends highly experienced, skilled, board-certified surgeons who are capable of delivering great results. Although the charges may vary depending on the experience of the surgeon, you can be assured that you are in safe and skilled hands when you choose bariatric surgery in India with IndiCure.
Depending on one's needs, men and women of all ages can benefit from multiple types of procedures. For example, Intra Gastric Balloon could be a cost-effective option for someone who is not very overweight and prefers a simple non-invasive procedure to treat obesity. IndiCure recommends you to explore the surgical options by consulting our expert bariatric surgeons.
Having your bariatric surgery in an accredited surgical facility by skilled and qualified medical staff is a critical factor. Moreover, the geographical location of this facility also affects the quote. But, IndiCure provides you with a projected estimate that will be all inclusive and affordable.
The surgery-related expenses include the pre-surgical and post-surgical expenses. The pre-surgical expenses are associated with the candidacy and the medical history of the patient. This also includes routine medical exams and tests to ensure you're a good fit for the desired procedure. Post-surgical expenses can include prescription medications, post-surgery, and follow-up consultations.
We at IndiCure, understand that you travel with a budget in mind and do not like to be greeted by surprises after arrival in India. We thus club all these expenses and give you the package cost that is inclusive and affordable at the same time.
Your case manager shall give you an estimated cost of your surgery after discussing your medical reports with the surgeon. The final cost, however, shall be confirmed after your consultation with the surgeon.
Years of Experience

Patients Assisted Worldwide
Countries Served

Most Preferred Medical Tourism Brand
Google Rating from Global Patients

Dr. Raman Goel
MBBS, MS, FICS, FIAGES, FALS
27+ Years of Experience
Dr. Ramen Goel, a highly qualified gastro-intestinal surgeon with more than 25 years of experience, is one of India's bariatric surgery pioneers. He has committed the past 20 years to performing a wide range of procedures using modern laparoscopic techniques. He is a member of the Surgical Review Corporation's International Review Committee, which awards Centers of Excellence in Bariatric Surgery.

Dr. Sanjay Borude
MBBS, MS, FICS, FIAGES, FALS, IFSO
30+ Years of Experience
Dr. Sanjay Borude is a highly renowned bariatric surgeon with more than 26 years of experience in the field. He has the LIMCA BOOK OF RECORDS for BARIATRIC SURGERY ON 11 MONTHS OLD BABY. Performed ASIA's first Google Eye' Bariatric Surgery with Google team. He is a pioneering surgeon in the field of obesity surgery in India.

Dr. H. V. Shivram
MBBS, MS, FICS, FRCS
27+ Years of Experience
Dr. Shivaram H V is one of the country's most renowned GI and bariatric surgeons, with a long list of groundbreaking studies and publications to his name. A huge number of national and international patients have benefited from his expertise in laparoscopic surgery, pancreatic surgery, gastro-intestinal surgery, and bariatric/metabolic surgery.

Wockhardt Hospital
Mumbai
Wockhardt Hospitals is the branch of the leading Wockhardt pharmaceutical company in India. The company is more than four decades old and is present in more than 20 countries around the globe. Wockhardt has 9 hospitals in India in Mumbai, Nagpur, Rajkot, Nashik, and Surat. Wockhardt hospitals have entered into a strategic alliance with Partners Medical International, USA, whereby the group has access to Harvard's expertise in clinical and surgical fields.

Fortis La Femme Hospital
Delhi
Fortis La Femme, founded in 2004, is a multi-specialty hospital that provides care for all periods of a woman's life, including birth, motherhood, menopause, and beyond. The hospital was named the winner of the ‘Most Popular Maternity Hospitals' category in Child magazine's Most Popular Awards 2013. More than 11,000 deliveries and 7,500 gynecological operations have been performed.
Watch this short video to understand how IndiCure supports international patients throughout their medical journey in India — from treatment planning and hospital coordination to recovery and travel support.
Bariatric surgery is a successful intervention and has been considered the most-effective long-term weapon in the treatment of obesity. It successfully offers substantial weight loss and decreases the health risks associated with Obesity. The surgery also greatly improves the quality of life.
Bariatric surgery is widely recommended for obese patients at high risk of morbidity and mortality, who have not been able to manage the weight loss even with an active lifestyle or medical help as well as the ones who are suffering from unresolved co-morbid conditions of obesity.
There is a whole range of endoscopic bariatric surgery procedures used as weight loss treatments. With a new generation of endoscopic equipment available, endoluminal bariatric weight loss surgery is gaining popularity as well, with up to 25-40% reduction in excess weight loss and around 60% resolution of comorbidities. Few of the available endoscopic bariatric surgery procedures include intragastric balloon, primary gastroplasty, and outlet reduction for failed gastric bypass, pouch creation, and endobarrier bypass sleeve.
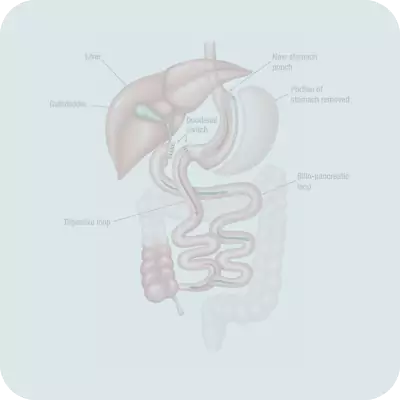
Surgery for weight loss is often the way to weight loss when the other methods have failed and the person is left with no other option. There are various techniques of weight loss surgery, though all of them work in three basic ways:
| Procedure Time | 2-4 hours depending on the type of procedure chosen |
|---|---|
| Anesthesia Type | General Anesthesia |
| Hospitalization | 1-3 Days |
| Stitch Removal | 7-8 Days |
| Recovery Time | 7-8 Days |
Bariatric surgery works well on individuals who fall in the category of "obese" or "morbidly obese", which means you have a BMI of 40 plus.
People with a BMI of more than 35 are also candidates for the surgery if they have comorbidities associated with obesity like diabetes, hypertension, sleep apnea, joint pain, etc.
The doctors would assess you before you are taken for the procedure. A few important factors that make you a good candidate for Bariatric surgery include the following:
Age: You should be between 18 and 60 years to undergo the procedure.
Weight: If your weight is 80% or more than your ideal body weight or you have a BMI of 40 plus; or 35 plus with comorbidities, you are a candidate.
Medical conditions: Obesity should not be because of medical conditions and you should not be suffering from or have been treated for serious medical conditions such as cancer, epilepsy, etc.
Lifestyle Changes: You should be committed to making lifelong changes to your lifestyle and eating habits.
Addictions: You should not be addicted to alcohol or other recreational drugs.
Preparation 1-2 weeks before Bariatric Surgery
You would need to follow a liquid diet plan for 7-14 days before the surgery.
The 1-2 week diet to be followed before the surgery would include protein shakes which would make the most part of your meal. You can have beverages but those should be sugar-free, non caffeinated and carbonated. Soup broth and vegetable juices and one or two servings of lean meat or vegetables are allowed.
The answer to the above question is definitely a big NO.
Who would like to pay and get a botched surgery or risk his/her life? Medical tourists come to India because they get quality healthcare services at an affordable cost.
While bariatric surgery cost in India definitely makes it one of the most popular destinations in the world, low cost is not the only reason why more and more people are opting for India as their preferred medical tourism destination.
Safe and effective bariatric surgery, modern technology, great services, excellent infrastructure, state of the art hospitals, personalized attention, world-renowned bariatric surgeons, no language barrier, and ease of travel are some of the factors which have attracted people from all across the globe for their bariatric surgery in India.
IndiCure is proud to associate with some of the best bariatric surgeons in India who have many years of experience in carrying out successful weight loss surgery. With IndiCure, you can be assured of personalized care and attention.
We at IndiCure completely understand your concerns and it is always our endeavor to provide the best outcome for every patient. Following is the list of questions you must ask before you embark on your journey for Bariatric Surgery in India.
Prepare to answer questions about your:

The answer is simple- You should choose to undergo bariatric surgery in India because of the many advantages that the country offers. Getting bariatric surgery in India with carefully chosen bariatric surgeons and clinics offers many advantages for bariatric surgery seekers abroad, a few of which are listed below -
Savings - Bariatric surgery cost in India is much lesser, about 60% to 90% cheaper, as compared to the cost of bariatric surgery in the UK, US, Canada, Australia or any other Western country. Bariatric surgery cost in India is as less as a third of what it costs to get the surgery done in any of these countries.
Best Bariatric Surgeons in the world - Bariatric surgeons in India are known for their skills and expertise all over the world. Not only are they trained at the best medical schools in the world, but the experience Indian bariatric surgeons have is also second to none.
Best bariatric surgery hospitals in India - The bariatric surgery hospitals and clinics that IndiCure chooses to associate with have state-of-the-art technology and zero MRSA rate which is even better than what you would find in many European countries.
No language barrier - English is the second official language of India. Surgeons, nurses, and other support staff at the hospital speak English, so communication is never a problem though not being used to a different accent may pose some difficulty at some times.
Incredible India - India is one of the most mystical countries on the earth, and has also come to be known as God's own country. It is a 'must-see destination' by all the well-known travel magazines and portals. People with completely different languages, cultures, religions all cordially living together as one country, is a unique experience to see.
Yes, absolutely. If you get your surgery done by a well-qualified and experienced surgeon, in a good surgical room, at a hospital that offers proper post-operative care; the risk of undergoing bariatric surgery anywhere in the world is just the same. So, whether you are in the US, UK, Australia, or Canada the risks remain the same keeping other factors constant.
The hospitals in India that we associate with are accredited, the surgeons' board-certified, and more experienced than their Western counterparts, and we give utmost attention to the fact that you have traveled from a faraway country and have special requirements.
We advise that you stay in India for a minimum of a week after you are discharged from the hospital to make sure you have healed adequately before you go back. All these factors make surgery in India a very safe proposition. We have in fact seen that with proper patient selection and proper precautions, the success rate of Bariatric surgery in India is much higher than in patients' home countries.
Pain is very subjective and varies from individual to individual. There definitely is some amount of pain and discomfort after any bariatric surgery, be it gastric bypass, gastric sleeve, or Lap-Band surgery.
Since bariatric surgery is mainly performed laparoscopically, the incisions given are quite small thereby leading to faster recovery and much lesser pain as compared to any open procedure, which involves significantly more discomfort and a longer stay in the hospital.
In general, pain is rarely a major concern following bariatric surgery. Pain medication can help you manage it. In a matter of days, most patients are off all pain medications and back to work.
Yes, absolutely!
You can lead a completely normal life after your weight loss surgery, in fact your quality of life will significantly improve post-surgery. What is however important is that you make positive changes in your diet and lifestyle after the surgery, which includes having smaller meals throughout the day, portion control, eating a high protein, low fat diet and having an active lifestyle.
Though every coin has 2 sides, when it comes to evaluating the pros and cons of bariatric surgery, the benefits usually outweigh the risks. Statistics show that the patients undergoing bariatric surgery procedures frequently have better health results and fewer obesity-related side effects, such as a lower risk of heart attack, joint pains, diabetes, hypertension, etc, and a better overall quality of life.
Significantly reduced prices, access to 24*7 nursing and medical care for at least 3-4 days after the surgery, personalized attention, and impeccable services are some of the additional benefits of undergoing bariatric surgery in India.
Non-invasive procedures like IGB will be done on a daycare basis and you would be discharged from the hospital the same day. Other procedures would require you to stay for 2-3 days at the hospital and another week in India before you can fly back.
Most people are able to return to light work after ten days and to heavy labor after six to eight weeks. The time of the return to work will depend upon the physical demands of the job and the rate of the recovery. Driving a car is usually permitted one week after surgery. Sexual activities may be resumed in week to ten days unless otherwise specified.
Exercise is important in recovery. Walking is one of the most effective forms of exercise for this purpose. Begin with very short walks several times a day and gradually increase the distance. Walking also improves muscle tone while you are losing weight. Do not, at first, engage in strenuous exercise. About six weeks after surgery, you should be able to tolerate all but the most strenuous exercises.
Bariatric surgery has the same risks associated as with any other major abdominal operation. Life-threatening complications or death are rare, occurring in less than 1% of patients. Such significant side effects as wound problems, difficulty in swallowing food, infections, and extreme nausea can occur in 5-10% of patients.
Your surgeon and dietician will slowly take you through different stages of diet after the surgery. It is in your best interest to follow the doctor's recommendation properly to let your body heal properly and avoid any post op complications. The diet is advised in a way that it keeps you nourished while you are still losing a lot of weight.
After the procedure, your doctor would advise you to sip fluids slowly and keep the portion very small so that you do not feel overfull at any time. You would be kept on a full liquid diet for a week or two after the surgery. It allows your stomach to heal well and avoid strain. You would be allowed to have only clear liquids for the first 1-2 days immediately after the surgery. This would include apple juice, chicken broth, beef broth, sugar-free gelatin, and artificially-sweetened non-carbonated beverages. Once the doctor and the dietitian are sure you can digest clear liquids well, your dietician would advise a full liquids diet for you. Full liquids include cream broth and soups, protein shakes, milk, yogurt, and sugar-free puddings.
This shall be followed by puréed foods after a couple of weeks. You must respect your body and proceed slowly to see what your body allows. You must keep the portion of your meals small and focus on high-protein foods. You would be advised to slowly add soft foods such as oatmeal and eggs.
Most people are able to start eating normal foods 4 - 8 weeks after the surgery. It will be important to choose healthy foods, eat slowly, chew food thoroughly, and to stop eating when you feel full.
This is how you can begin your journey to a new and improved you or simply put, weight loss surgery in India:
Contact us through mail or call us at the numbers provided above. One of our representatives will get in touch with you.
You would be asked for a few details to assess your candidacy for bariatric surgery. You can also fill in the form.
We shall get back to you with our expert bariatric surgeon's opinion, exact cost, and complete details about your surgery.
You can ask any number of questions and we shall get answers to all your queries through our expert bariatric surgeons in India.
You can then finalize your dates and we help you with visas, bookings, and further steps.
Undergoing bariatric surgery is a life-changing procedure and should be considered carefully. The following steps will help you prepare for surgery and the changes that you will go through.
Your medical information is handled confidentially and is used only for patient support and treatment coordination.
Beyond treatment coordination, IndiCure also helps international patients experience a more comfortable and meaningful healthcare journey in India.

We assist patients in accessing wellness retreats focused on relaxation, restorative care, and recovery support.
Know More >>
IndiCure helps patients access Ayurveda programs through selected wellness centers and experienced practitioners.
Know More >>
From cultural experiences and historical destinations to local guidance during recovery, IndiCure helps international visitors experience India in a comfortable and supportive environment.
Know More >>With over 15 years of experience, IndiCure supports international patients by coordinating both the clinical and travel aspects of treatment in India. We work with a network of board-certified surgeons and JCI- and NABH-accredited hospitals that follow established safety and clinical protocols.
Our team manages each stage of the journey, including medical evaluations, visa assistance, travel planning, and accommodation arrangements—providing a structured and transparent process from initial consultation through follow-up care.
The content provided on this website is intended for general educational purposes only and does not constitute professional medical advice, diagnosis, or treatment. While we maintain a comprehensive editorial policy to ensure the accuracy and reliability of our information, this content should not be utilized as a substitute for professional clinical care.
Individual Results: All "before and after" photographs are illustrative examples of potential outcomes; actual surgical results vary significantly by individual.
Mandatory Consultation: We strongly advise a personal, in-person evaluation with a board-certified surgeon to assess your specific medical needs and realistic procedural goals.
Surgical Risk: It is vital to maintain realistic expectations and fully understand potential complications before electing for surgery.